Orthopedic trauma surgery comprises some of the most complicated and difficult surgery encountered by the orthopedic surgeon in practice. A variety of techniques may be employed to stabilize injuries and the patient. Unfortunately, through no fault of the surgeon or patient, orthopedic complications may occur such as implant breakage, malunion and nonunion.
Post Traumatic Residuals produce abnormal alterations of the normal mechanics of the Musculoskeletal system. Depending on the original injury, they may occur anywhere and disrupt the normal function of any joint.
Certain injuries around the hip are predisposed to such problems. The femoral neck fracture was named “The Unsolved Fracture” precisely because of the common problems associated with this injury. Two of the more common problems encountered with this injury are avascular necrosis of the femoral head and nonunion of the femoral neck.
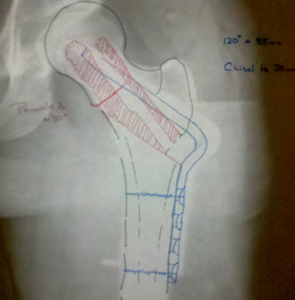
Proximal femoral deformities as the result of treatment of femoral fractures can be problematic, an angular malunion of the femur may cause problems with gait or healing of the fracture. Retained broken hardware may create challenges for subsequent reconstruction. These patients typically have hip pain, slight bowing of the leg, and shortening of the involved extremity. The end result is a mechanical disturbance which left untreated contributes to continued disability and pain in the patient’s life.